

 By Usama Abbasi, PhD Candidate, Kizhakkedathu Lab
By Usama Abbasi, PhD Candidate, Kizhakkedathu Lab
Myelodysplastic syndrome (MDS) represents a group of diseases often referred to as bone marrow failure, which usually develops in older people. In Canada alone, up to 6,000 new cases are diagnosed each year. The median survival for these patients ranges from 0.5 to 6 years after diagnosis.
In healthy individuals, the bone marrow produces immature blood cells, which subsequently mature into red blood cells (RBCs), white blood cells, and platelets. In patients with MDS, however, cell development and maturation is disrupted in the bone marrow and results in insufficient numbers of healthy blood cells in circulation. As a result, the majority of MDS patients develop severe anemia, leukopenia, and thrombocytopenia (low platelets) and thus may require frequent blood transfusions.
Due to the diversity of MDS, the standard of care for patients is constantly changing. Although more aggressive forms of treatment are available for high-risk subgroups, such as stem cell transplantation, chemotherapy, or hypomethylating agents, the mainstay of treatment is supportive care. This consists of transfusions which temporarily elevate the number of healthy cells in circulation – RBC or platelet transfusions.
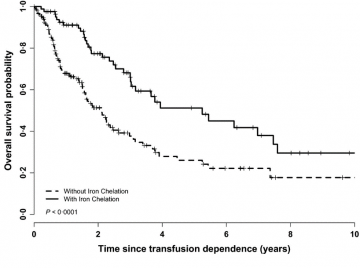
Figure 1. Overall survival from red blood cell transfusion dependence by receipt of iron chelation therapy in all patients
A major side effect of repeated RBC transfusions is the development of transfusion-dependent secondary iron overload. Humans are unique in that they lack a proper iron excretion pathway while maintaining 3 to 5 grams of iron throughout their lifespans. Iron is an essential element; however, it has enormous damaging potential when present in excess – it catalyzes free radical generation. Each RBC transfusion introduces an additional 250 milligrams of iron into the circulation. Consequently, the increased iron burden eventually causes ‘iron overload,’ imparting toxicity to the transfusion recipient; organ dysfunction is a major complication, with cardiac- and hepatic- failure accounting for many deaths.
In the October 2017 issue of the British Journal of Haematology, CBR investigator and staff hematologist, Dr. Heather Leitch (St. Paul’s Hospital), and co-workers analyzed the Canadian MDS Registry to evaluate whether there is superior survival in MDS patients receiving iron chelation therapy (ICT). It is worth noting that various MDS registries previously indicated that RBC transfusion dependence – and subsequent iron overload – are associated with inferior overall patient survival. Further, analyses have documented an association between receiving iron chelation therapy and superior overall survival. All of these studies of ICT in MDS to date, however, did not control for potentially confounding variables.
A review was conducted by Leitch and co-workers of prospectively collected data accounting for patient-related factors, such as patient frailty, comorbidities and pre-existing disabilities. A match pair analysis was also performed to account for differences in baseline characteristics and other disease-modifying drug regimens. In the article, the authors concluded that “although patient-related factors did not differ between iron chelation therapy and non-iron chelation therapy patients, the receipt of chelation was independently associated with superior survival.” (Figure 1.)
This prospective study provides additional evidence in support of chelation therapy conferring clinical benefit to transfusion-dependent MDS patients, although Dr. Leitch and coworkers recognize that a randomized, placebo-controlled clinical trial will be able to definitively address the pros and cons of chelation in MDS.